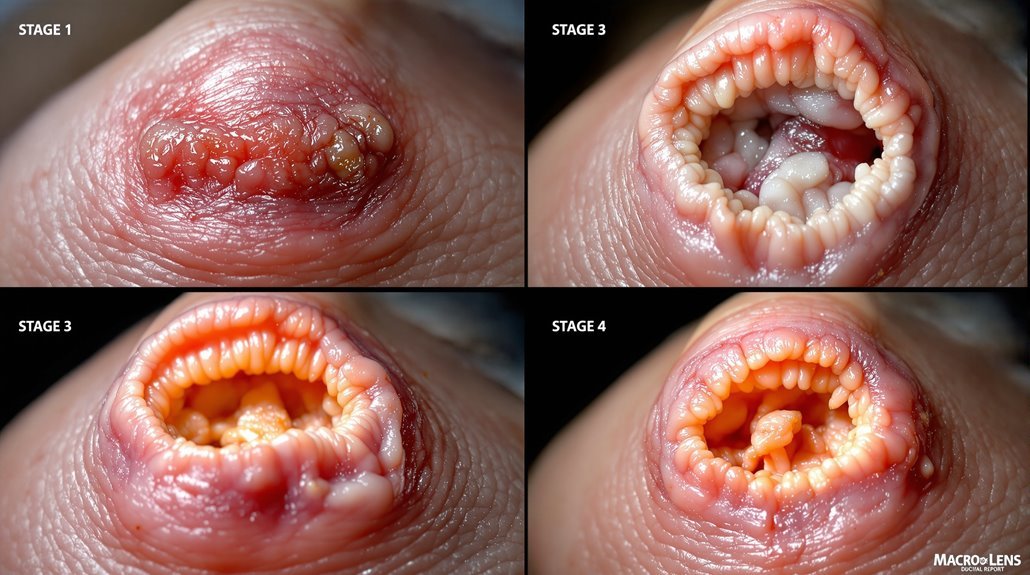
You need to recognize pressure ulcer stages quickly because they progress rapidly through your skin layers. Your skin first shows non-blanchable redness that doesn’t blanch with pressure—that’s stage one. Stage two involves partial-thickness loss exposing the dermis. Stage three penetrates all skin layers into subcutaneous tissue. Stage four causes extensive tissue damage; deep tissue injuries hide dangerous damage beneath the surface. Each stage demands different prevention strategies that become increasingly critical for your recovery.
Key Takeaways
- Stage 1 shows non-blanchable redness over bony prominences; skin remains intact but indicates compromised blood flow.
- Stage 2 involves partial-thickness skin loss exposing dermis, appearing as an open sore or blister.
- Stage 3 represents full-thickness tissue loss penetrating all skin layers, exposing subcutaneous tissue beneath.
- Deep tissue injuries show non-blanchable deep red, maroon, or purple discoloration with potential blood-filled blisters.
- Unstageable injuries mask full-thickness loss beneath slough or eschar, requiring frequent skin assessments.
What Are Pressure Ulcers?
Pressure ulcers—commonly called bedsores or decubitus ulcers—are localized injuries to your skin and deeper tissues that develop when prolonged pressure restricts blood flow, typically over bony prominences like your heels, sacrum, and elbows.
These painful wounds manifest as non-blanchable erythema in early stages, progressing to significant tissue loss if left untreated.
Understanding pressure ulcer risk factors is essential for effective nursing care. Immobility stands as the primary risk factor, particularly affecting individuals confined to beds and wheelchairs.
Additional factors include poor nutrition, moisture exposure, and advanced age.
Prevention strategies prove far more effective than treatment. You’ll implement regular repositioning, utilize specialized pressure-relief mattresses, and conduct daily skin inspections.
These nursing interventions directly reduce ulcer formation and improve patient outcomes in vulnerable populations.
Stage 1: Non-Blanchable Erythema
When your skin remains intact but displays non-blanchable erythema—localized redness that doesn’t blanch (turn white) when you press it—you’re experiencing a Stage 1 pressure ulcer. At this stage, you’ve detected compromised blood flow to a localized area, typically over bony prominences like the sacrum and heels.
Your skin may feel warmer or cooler than surrounding tissue, with changes in color or texture. In individuals with darker skin tones, you might observe persistent blue or purple hues instead of typical redness. Early detection is absolutely critical—Stage 1 represents the first sign of potential skin breakdown and offers your best window for intervention and prevention.
| Assessment Focus | Key Indicators |
|---|---|
| High-Risk Areas | Sacrum, heels, hips |
| Skin Changes | Temperature, texture, color variations |
| Timeline | Early intervention prevents progression |
Regular assessment of vulnerable areas prevents advancement to more severe stages. Implement pressure relief measures immediately upon recognition.
Stage 2: Partial-Thickness Skin Loss

Your skin’s protective barrier ruptures at Stage 2, moving beyond the redness of Stage 1 into actual tissue loss.
You’re experiencing partial-thickness skin loss that exposes the dermis beneath your epidermis, creating a shallow wound with a viable wound bed. The affected area appears red and swollen, often tender to touch, indicating compromised skin integrity.
Partial-thickness skin loss exposes your dermis, creating a shallow wound with red, swollen, tender skin indicating compromised skin integrity.
This stage demands prompt treatment to prevent progression to deeper tissue involvement. You’ll typically see the wound present as an open sore, blister, or abrasion—all signs that your skin’s protective layers have broken down.
Developing an effective care plan immediately is critical. Without intervention, this partial-thickness wound deteriorates into more severe stages, affecting deeper tissues.
Your commitment to addressing Stage 2 pressure ulcers now protects against serious complications.
Stage 3: Full-Thickness Tissue Loss
Deterioration reaches a critical point at Stage 3: the wound now penetrates all skin layers and exposes the subcutaneous tissue beneath.
You’re observing full-thickness tissue loss, where the ulcer extends through skin and fat into subcutaneous tissue. The wound bed may display necrotic tissue with granulation tissue as healing begins.
Stage 3 pressure ulcers develop from prolonged pressure on bony prominences, especially in individuals with limited mobility or sensation.
You must monitor carefully for infection signs—increased drainage, odor, or warmth—which compromise recovery.
Your advanced wound care should include regular debridement to remove dead tissue and specialized dressings.
Implementing pressure relief measures remains essential.
Your careful assessment and intervention support tissue regeneration and prevent progression to more severe stages requiring surgical intervention.
Stage 4: Extensive Tissue Damage

Stage 4 pressure ulcers represent the most severe form of tissue damage, extending through all skin layers and exposing fascia, muscle, or bone.
You’ll observe significant damage characterized by full-thickness skin loss, with visible tendons, muscles, and bone. These wounds display tissue necrosis with black discolored areas. The sore may emit a foul odor and discharge pus, suggesting infections.
Full-thickness tissue loss reveals underlying muscle and bone with tissue necrosis, foul odor, and pus drainage indicating infection.
Without prompt intervention, these ulcers progress to life-threatening conditions like sepsis or osteomyelitis. Accurate staging is essential for determining appropriate wound care strategies.
Your treatment approach requires surgical interventions including debridement and skin grafting. Early detection of earlier-stage ulcers prevents progression to this critical stage.
Special Types: Deep Tissue and Unstageable Injuries
While Stage IV pressure ulcers represent the most visible form of advanced tissue damage, two other classifications—deep tissue injuries and unstageable wounds—present equally serious threats that don’t always fit the traditional staging framework.
Deep Tissue Pressure Injury manifests as non-blanchable deep red, maroon, or purple discoloration indicating underlying tissue damage. You’ll observe blood-filled blisters that mask serious damage beneath intact skin. Because DTPI evolves rapidly over time, thorough skin assessments prove absolutely essential for early detection and proper intervention.
Unstageable injuries completely hide full-thickness loss beneath slough or eschar. You can’t determine the wound’s true extent until necrotic tissue separates, considerably complicating treatment decisions and increasing complications like serious infection risks. Both injury types require careful monitoring to promote ideal healing outcomes.
| Category | Deep Tissue Injury | Unstageable Injury |
|---|---|---|
| Appearance | Purple/maroon discoloration | Hidden by slough/eschar |
| Detection Challenge | May appear intact initially | Wound extent obscured |
| Complication Risk | High infection potential | Critical deterioration risk |
| Assessment Need | Frequent skin assessments | Careful ongoing monitoring |
| Healing Focus | Pressure relief & dressing | Staged tissue separation management |
Causes and Risk Factors
When pressure concentrates over bony prominences during prolonged immobilization, blood flow becomes restricted and tissue damage begins—the hallmark of pressure ulcer development.
You’ll find that multiple risk factors compound this danger. Neurologic diseases and decreased consciousness impair sensory perception, leaving patients unable to detect discomfort or shift positions. Spinal cord injuries and nursing home residents face particularly high vulnerability.
Beyond prolonged pressure, skin shear and friction damage the epidermis, creating microscopic tears that weaken skin integrity. Excessive moisture from body fluids further compromises this barrier.
Understanding these interconnected risk factors enables you to implement preventive measures effectively. Regular skin assessments and risk evaluation tools like the Braden Scale facilitate early identification of at-risk individuals, allowing timely intervention to prevent pressure ulcers before development.
Prevention and Management Strategies
Since effective prevention and management can’t rely on a single strategy, you’ll need to combine multiple interventions addressing pressure relief, tissue assessment, and care coordination.
Regular repositioning every two hours for bedridden patients and every 15 minutes for wheelchair users forms the foundation of prevention strategies. Implement pressure-relieving cushions and specialized support surfaces to redistribute pressure on vulnerable areas.
Regular repositioning every two hours, combined with pressure-relieving surfaces, forms the foundation of pressure ulcer prevention.
Daily skin assessments help you detect early signs at common pressure ulcer sites like the sacrum, heels, and elbows. For high-risk patients, establish a structured care plan incorporating skin care, moisture management, and nutritional support.
Adequate protein and hydration enhance tissue perfusion, reducing pressure ulcer development. By coordinating repositioning, assessments, equipment, and nutrition, you provide thorough care preventing complications and protecting your patients’ skin integrity.
Conclusion
You’ll recognize that understanding pressure ulcer staging helps you identify problems early and prevent serious complications. By knowing what each stage looks like, you can spot the warning signs—from early redness to severe tissue damage with exposed bone. You’ll want to focus on prevention through regular repositioning, proper skin care, and maintaining patient mobility, especially for those at high-risk. You’re empowered to make a real difference in outcomes when you take these stages seriously and respond promptly.

